For health plans and managed care organizations, incontinence remains a vastly under-recognized driver of cost, risk, and member dissatisfaction, yet it is also a modifiable lever to improve performance. When addressed proactively, continence management can reduce avoidable utilization, delay institutionalization, and improve member experience while strengthening quality and financial outcomes for Medicaid, Medicare Advantage, and other risk-bearing plans. [1][2]
The hidden cost of incontinence
Incontinence is often framed as a quality-of-life concern rather than a core cost and risk issue, but its downstream impact on healthcare utilization is substantial. Recent analyses show that urinary incontinence and overactive bladder together are associated with tens of billions of dollars in annual costs in the United States, driven by higher rates of outpatient visits, hospitalizations, and prescription use compared with matched adults without incontinence. For payers, these costs are compounded by sequelae such as falls, fractures, skin breakdown, and infections, which are frequently preventable with systematic continence management. [1][2][3][4]
The payer perspective: Why continence management matters
From a payer standpoint, incontinence-related costs extend far beyond supplies to include increased use of home health, emergency services, and skilled nursing facilities. Members with stress or mixed urinary incontinence incur markedly higher total costs over multi-year periods than controls, reflecting more frequent physician visits, hospital care, and medication use. In addition, incontinence-related falls and fractures create another layer of financial exposure, given the high acute and post-acute costs associated with hip fractures and other serious injuries in older adults. [1][2][4]
Indirect costs are equally important. Untreated or poorly managed incontinence contributes to falls, skin breakdown, and urinary tract infections, each of which can trigger a cascade of escalations from ED visits to hospital admissions and long-term care placement. These complications drive utilization in high-cost settings and often result in permanent loss of independence, particularly for older adults with multiple chronic conditions. For plans that serve a high proportion of frail or dually eligible members, these dynamics can significantly influence total cost of care and medical loss ratios. [1][4][5][6]
Incontinence and risk of institutionalization
Incontinence is a well-established predictor of functional decline and more supported living arrangements. Studies in older adults show that urinary incontinence and especially dual incontinence (urinary and fecal) are associated with higher likelihood of transitioning to more intensive care settings within a year, even after accounting for age and comorbidities. In nursing homes, a large proportion of residents who are continent at admission develop dual incontinence over the first one to two years, highlighting both the scale of the problem and the opportunity for proactive interventions. [1][7][6]
For Medicaid and Medicare Advantage plans, each avoidable admission or prolonged stay in a nursing facility represents a major cost center. Because Medicaid remains the primary payer for long-term services and supports, preventable institutionalization driven by incontinence has implications for both state budgets and the financial performance of D-SNPs and other integrated plans. Addressing continence more systematically can therefore align clinical and financial goals by supporting community tenure while reducing dependence on institutional care.[1][5][7]
Falls, fractures, and safety risks
Incontinence is closely linked with fall risk, particularly in older adults who experience urgency, nocturia, and mobility limitations. Urgency-related rushing to the bathroom, especially at night, contributes to falls, and nocturia has been associated with increased risks of both falls and fractures in observational studies. Fragility fractures following falls have profound consequences, including functional decline, loss of independence, and elevated mortality in the year after injury. [1][4][6][8]
The associated costs are significant. Hip fractures in older adults result in high acute care expenditures and extended post-acute rehabilitation, along with increased likelihood of long-term institutionalization. When incontinence is not addressed, plans face recurring costs from ED visits, hospital stays, and readmissions, as well as ongoing expenditures for post-acute and long-term care. Integrating continence management into fall prevention programs gives payers a practical way to reduce these events while improving safety and quality of life for members. [1][4][5][8]
Quality of life, independence, and member retention
Beyond utilization and cost, incontinence exerts a powerful effect on members’ daily lives, social engagement, and emotional well-being. Members with incontinence often limit activities, avoid social situations, and feel a loss of dignity, which can worsen depression, anxiety, and adherence to other aspects of chronic disease management. Effective continence support, including appropriate products, education, and care coordination, helps restore autonomy and confidence, which are central to aging in place and maintaining social supports. [1][2][5]
For health plans, these member-level impacts translate directly into satisfaction, retention, and perception of plan responsiveness to real-world needs. In Medicare Advantage, better experiences among older adults can support performance on CAHPS and Care for Older Adults-related measures, feeding into STAR ratings and associated bonus payments. Proactive attention to continence is therefore not just a clinical courtesy but a differentiating feature of member-centered plan design. [1][5]
Impact on Medicare Special Needs Plans
The burden and strategic importance of incontinence are particularly pronounced in Medicare Special Needs Plans. Institutional SNPs (I-SNPs) serve nursing home residents, a population with high rates of incontinence and dual incontinence, and therefore a high incidence of skin breakdown, infections, and falls. For these plans, integrating continence protocols into routine assessments and daily care can reduce avoidable hospitalizations, pressure injuries, and ED visits, improving both quality metrics and per-member cost trends. [1][5][7]
Dual Eligible SNPs (D-SNPs) care for individuals served by both Medicare and Medicaid, many of whom have complex functional and social needs that place them at heightened risk of institutionalization. In this context, unaddressed incontinence can be a tipping point from community living to nursing facility placement, with long-term consequences for both programs. Chronic Condition SNPs (C-SNPs) managing members with conditions like diabetes, heart failure, and neurologic disease also see higher prevalence of incontinence related to comorbidities and medications, making continence management an important component of comprehensive chronic care.[1][2][5][7]
The strategic opportunity for plans
When viewed strategically, continence management becomes a cross-cutting lever that touches utilization, risk mitigation, member experience, and competitive differentiation. Plans that systematically identify members with incontinence, optimize supplies and clinical support, and integrate continence into fall prevention and care management programs can reduce total cost of care while improving outcomes. Claims analytics, assessment data, and predictive modeling can be used to flag at-risk members, including those with frequent UTIs, falls, or nocturia, and target interventions before costly complications occur. [1][2][5]
Operationally, turnkey continence programs can also lessen administrative burden. Each preventable fall, UTI, or pressure ulcer generates not only medical expenses but also internal workload in the form of authorizations, transitions of care, appeals, and case management time. By shifting from reactive authorization of downstream care to upstream continence interventions, plans can free clinical and administrative staff to focus on higher-value work and complex cases. [1][5]
Aeroflow Health’s approach to continence management
Aeroflow Health partners with health plans to convert fragmented, reactive incontinence management into a proactive, data-driven strategy. The model begins with early identification, using data analytics and member outreach to surface individuals exhibiting signs of incontinence or related complications before they incur avoidable high-cost events. Once identified, members receive tailored continence supply programs matched to their functional status, environment, and preferences, reducing leakage, skin breakdown, and the need for higher-acuity care.[1][5]
This product optimization is combined with integration into existing case management, care coordination, and fall prevention workflows, minimizing disruption for plan teams. For example, continence assessments and product reviews can be embedded into fall risk evaluations or post-discharge follow-ups, creating a unified approach to safety and independence. Aeroflow’s model emphasizes education and support for members and caregivers, helping them use products correctly, manage symptoms, and communicate changes in status that might signal evolving risk. [1][4]
Linking continence to falls and quality
A key component of Aeroflow Health’s strategy is explicit alignment with fall prevention initiatives. Because nocturia, urgency, and mobility challenges combine to drive nighttime falls, interventions that stabilize continence can meaningfully lower risk. Plans can use claims and assessment data to identify high-risk members, deploy targeted continence supplies and home safety modifications, and then monitor falls, ED visits, and fractures over time to demonstrate impact.[1][4][8]
These efforts also support performance on quality measures related to functional status, care coordination, and member experience. By improving continence and related outcomes, plans can positively influence both clinical quality metrics and patient-reported measures that feed STAR ratings and bonuses. In competitive markets, a visible, well-executed continence program becomes part of the plan’s value proposition to members, caregivers, and providers.
From overlooked burden to strategic lever
The burden of untreated or poorly managed incontinence is too great for members who lose independence and dignity, for caregivers who struggle with day-to-day care, and for health plans facing avoidable high-cost utilization and institutionalization. Treating continence as a strategic priority rather than a peripheral benefit allows plans to reduce total cost of care, support aging in place, and enhance member satisfaction and loyalty. Through data-driven identification, optimized supplies, and integrated care coordination, partners such as Aeroflow Health enable payers to move from reactive management of incontinence-related complications to proactive, measurable improvement in outcomes and financial performance. [1][2][5]
Are you a health plan interested in learning how we can support your members while lowering your total cost of care? Contact us here to learn more.

Dr. Mike Cantor is a geriatrician and attorney who has extensive experience designing and implementing value-based care, quality improvement, and care management programs for healthcare providers and health plans. He works as a fractional (part-time) Chief Medical Advisor for Aeroflow Healthcare and other technology-enabled health services companies, value-based care organizations, and digital health companies. Previous roles include: CMO for Uber Health, the logistics and transportation company, Bright Health Plan, an innovative health insurer; CMO for CareCentrix, a leading outsourced home health, durable medical equipment, and post- acute care benefits manager acquired by Walgreens; and CMO for the New England Quality Care Alliance (NEQCA), the physician network affiliated with Tufts Medical Center, where he implemented network-wide quality improvement and care management programs for 150,000 managed care lives. He trained in internal medicine at Beth Israel Hospital in Boston and did his geriatrics fellowship at Harvard Medical School. He has degrees in law and medicine from the University of Illinois.
- 1. https://pmc.ncbi.nlm.nih.gov/articles/PMC9542745/
- 2. https://pmc.ncbi.nlm.nih.gov/articles/PMC10397717/
- 3. https://pmc.ncbi.nlm.nih.gov/articles/PMC6288612/
- 4. https://aahomecare.org/files/galleries/Incontinence_Quality_Standards_White_Paper_FINAL_06_23_20.pdf
- 5. https://pmc.ncbi.nlm.nih.gov/articles/PMC10811924/
- 6. https://pmc.ncbi.nlm.nih.gov/articles/PMC5640456/
- 7. https://www.auajournals.org/doi/10.1097/JU.0000000000000459
- 8. https://www.sciencedirect.com/science/article/abs/pii/S0029784401014648
- 9. https://onlinelibrary.wiley.com/doi/full/10.1002/nau.24989
- 10. https://www.auajournals.org/doi/10.1097/JU.0000000000000866.03


























































































































 What is an Inhaler?
What is an Inhaler? Rescue inhaler: a rescue or quick-relief inhaler is used to help get your breathing back under control in the event of wheezing, shortness of breath, chest tightness, or coughing.
Rescue inhaler: a rescue or quick-relief inhaler is used to help get your breathing back under control in the event of wheezing, shortness of breath, chest tightness, or coughing.




 If your child suffers from a respiratory disorder such as chronic bronchitis, asthma, cystic fibrosis they may benefit from using a nebulizer instead of an inhaler. They are often prescribed when children are too little or afraid to use inhalers.
If your child suffers from a respiratory disorder such as chronic bronchitis, asthma, cystic fibrosis they may benefit from using a nebulizer instead of an inhaler. They are often prescribed when children are too little or afraid to use inhalers.












 While many children are able to use a quick-relief inhaler to ease asthma symptoms, sometimes nebulizers are easy to use. Children can be afraid to use inhalers or medicine can be hard to aim with them. Make sure your child is able to use an inhaler correctly by sending medicine directly to their lungs before they stop using their nebulizer.
While many children are able to use a quick-relief inhaler to ease asthma symptoms, sometimes nebulizers are easy to use. Children can be afraid to use inhalers or medicine can be hard to aim with them. Make sure your child is able to use an inhaler correctly by sending medicine directly to their lungs before they stop using their nebulizer.








 You are responsible for paying the other 20%. However, if you are also enrolled in a Medicare supplement, then your supplement policy will generally pay some or all of this coinsurance for you depending on which plan you purchased.
You are responsible for paying the other 20%. However, if you are also enrolled in a Medicare supplement, then your supplement policy will generally pay some or all of this coinsurance for you depending on which plan you purchased.

 If you’re suffering from lymphedema we can help you qualify to receive a lymphedema pump through insurance. Simply fill out our online form and we will review your coverage and options with you. Then we will submit all of the necessary paperwork to your providers and guide you through the process to qualify for the medical supplies you need.
If you’re suffering from lymphedema we can help you qualify to receive a lymphedema pump through insurance. Simply fill out our online form and we will review your coverage and options with you. Then we will submit all of the necessary paperwork to your providers and guide you through the process to qualify for the medical supplies you need. Pollen is everywhere you look in the spring and summer. For months flowers, trees, grasses, grains, and more release pollen in the air, causing people to sniffle, sneeze, and wheeze. On top of that, even if you think you’re safe, away from all of the blooms, pollen can travel for miles and set off your histamines. Then physical activities that involve running through the grass or using your lawnmower can stir up these particles, causing them to settle on multiple surfaces from your clothes, the walls, vehicles, and more.
Pollen is everywhere you look in the spring and summer. For months flowers, trees, grasses, grains, and more release pollen in the air, causing people to sniffle, sneeze, and wheeze. On top of that, even if you think you’re safe, away from all of the blooms, pollen can travel for miles and set off your histamines. Then physical activities that involve running through the grass or using your lawnmower can stir up these particles, causing them to settle on multiple surfaces from your clothes, the walls, vehicles, and more.

 Nebulizers are essentially an asthma machine even though they provide breathing treatments for a variety of lung conditions such as chronic bronchitis, chronic obstructive pulmonary disease (COPD), cystic fibrosis, and more.
Nebulizers are essentially an asthma machine even though they provide breathing treatments for a variety of lung conditions such as chronic bronchitis, chronic obstructive pulmonary disease (COPD), cystic fibrosis, and more. Typical inhalable nebulizer medicines include:
Typical inhalable nebulizer medicines include:  Symptoms of
Symptoms of  Even though wearing compression stockings during the day can help with sleep apnea, you still want to use your
Even though wearing compression stockings during the day can help with sleep apnea, you still want to use your  Your doctor will prescribe compression stockings if you need them for any reason. They will also measure your legs to determine what size and amount of pressure you need for daily use. Compression stockings with a lower pressure setting usually don’t require a doctor’s prescription.
Your doctor will prescribe compression stockings if you need them for any reason. They will also measure your legs to determine what size and amount of pressure you need for daily use. Compression stockings with a lower pressure setting usually don’t require a doctor’s prescription. When you choose a Durable Medical Equipment supplier, you want to make sure that getting your equipment is as seamless as possible. Durable Medical Equipment (DME) is any equipment that provides therapeutic benefits to a patient in need because of certain medical conditions and/or illnesses. Sometimes, patients urgently need this medical equipment. This is why it’s so important to understand Medicare’s DME requirements.
When you choose a Durable Medical Equipment supplier, you want to make sure that getting your equipment is as seamless as possible. Durable Medical Equipment (DME) is any equipment that provides therapeutic benefits to a patient in need because of certain medical conditions and/or illnesses. Sometimes, patients urgently need this medical equipment. This is why it’s so important to understand Medicare’s DME requirements.
 A Face-to-Face visit is also required for some wheelchairs, including power wheelchairs and motorized wheelchairs. The distinction between a power wheelchair and a power mobility device is that the wheelchair is defined as being controlled by a joystick or an electronic device rather than a tiller. Generally, they are needed by those who cannot use a cane, walker, or standard manual wheelchair. They are easily controlled with the use of a joystick and can be maneuvered in tight spaces around the home to assist those with mobility issues.
A Face-to-Face visit is also required for some wheelchairs, including power wheelchairs and motorized wheelchairs. The distinction between a power wheelchair and a power mobility device is that the wheelchair is defined as being controlled by a joystick or an electronic device rather than a tiller. Generally, they are needed by those who cannot use a cane, walker, or standard manual wheelchair. They are easily controlled with the use of a joystick and can be maneuvered in tight spaces around the home to assist those with mobility issues. Hospital beds offer patient comfort and mobility because caregivers can wheel them to different areas of the home. Some are even electric to provide patients with the option of easily changing positions during the day when mobility issues and other conditions place them on bed rest.
Hospital beds offer patient comfort and mobility because caregivers can wheel them to different areas of the home. Some are even electric to provide patients with the option of easily changing positions during the day when mobility issues and other conditions place them on bed rest.  An inhaler spacer is a small device that is added to the end of an inhaler to assist with properly inhaling the medication. They are tubes that hold the medicine for you to inhale if inhalers seem to puff too quickly.
An inhaler spacer is a small device that is added to the end of an inhaler to assist with properly inhaling the medication. They are tubes that hold the medicine for you to inhale if inhalers seem to puff too quickly. A
A  This may sound similar to a herniated disc, but it’s distinct in the sense that
This may sound similar to a herniated disc, but it’s distinct in the sense that  Take care of your back with hot and cold compresses.
Take care of your back with hot and cold compresses.


 What are some examples of aging in place design? Some Aging in Place design elements would be the inclusion of wider hallways and doorways, sufficient lighting that can adjust to aging eyes, handles and grab bars selected for ease of use, and cabinet and appliance placement planned for limited mobility use. A curbless shower makes it easy for anyone and the extra lighting helps aging eyes.
What are some examples of aging in place design? Some Aging in Place design elements would be the inclusion of wider hallways and doorways, sufficient lighting that can adjust to aging eyes, handles and grab bars selected for ease of use, and cabinet and appliance placement planned for limited mobility use. A curbless shower makes it easy for anyone and the extra lighting helps aging eyes.


 Home Oxygen Concentrator – A home oxygen concentrator (HOC) concentrates air from the surrounding room into purified oxygen for medical use within a home setting. Instead of needing oxygen tanks they can be used anywhere. HOC devices generally plug into standard outlets and weigh between 30 to 55 pounds, providing some portability.
Home Oxygen Concentrator – A home oxygen concentrator (HOC) concentrates air from the surrounding room into purified oxygen for medical use within a home setting. Instead of needing oxygen tanks they can be used anywhere. HOC devices generally plug into standard outlets and weigh between 30 to 55 pounds, providing some portability.


 Has the body prepares to give birth, the
Has the body prepares to give birth, the 




 Take the stairs instead of the elevator.
Take the stairs instead of the elevator.



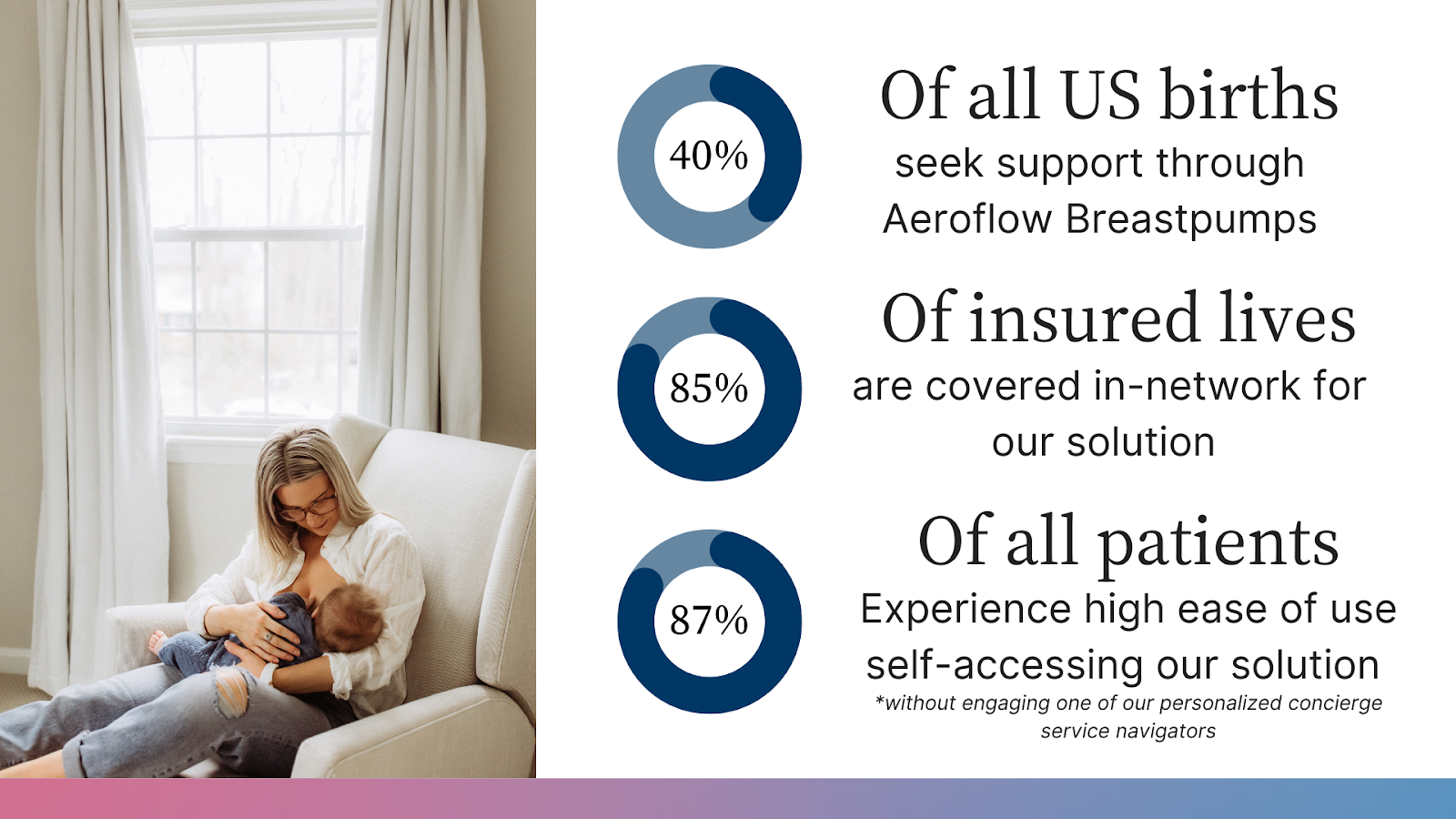
 Aeroflow Breastpumps was able to:
Aeroflow Breastpumps was able to:  Edema is still somewhat of a mystery but is generally attributed to changing estrogen and progesterone levels. Edema often arises during pregnancy as the growing baby and expanding uterus will put pressure on the vena cava vein running down the right side of the body. This causes blood flow to slow and excess fluid to leak into the tissue of the ankles and feet.
Edema is still somewhat of a mystery but is generally attributed to changing estrogen and progesterone levels. Edema often arises during pregnancy as the growing baby and expanding uterus will put pressure on the vena cava vein running down the right side of the body. This causes blood flow to slow and excess fluid to leak into the tissue of the ankles and feet. You should only worry when you begin to experience symptoms beyond mild to moderate swelling and discomfort. Intense pain in the legs or frequent headaches can be a sign of high blood pressure. If the swelling is located in one area or is on one side of the body, this can be a sign of a blood clot and should be immediately addressed by a physician.
You should only worry when you begin to experience symptoms beyond mild to moderate swelling and discomfort. Intense pain in the legs or frequent headaches can be a sign of high blood pressure. If the swelling is located in one area or is on one side of the body, this can be a sign of a blood clot and should be immediately addressed by a physician.
 The higher the compression, the tighter the stocking will feel. The pressure stocking levels usually range from light (10-15 mmHg) to firm (30-40 mmHg). Your doctor can prescribe a higher level of compression if any of these compression levels do not reduce your swelling.
The higher the compression, the tighter the stocking will feel. The pressure stocking levels usually range from light (10-15 mmHg) to firm (30-40 mmHg). Your doctor can prescribe a higher level of compression if any of these compression levels do not reduce your swelling. Medicare Part A covers inpatient hospital care, hospice, surgery,
Medicare Part A covers inpatient hospital care, hospice, surgery,  Remember the open enrollment period is for people who are already enrolled in Medicare. If you need to enroll, do so during your initial enrollment period which is 3 months before your 65th birthday, the month of your 65th birthday, or the 3 months after.
Remember the open enrollment period is for people who are already enrolled in Medicare. If you need to enroll, do so during your initial enrollment period which is 3 months before your 65th birthday, the month of your 65th birthday, or the 3 months after. Opioid Side Effects:
Opioid Side Effects:  Whether you need a back brace for posture for lower back pain, you’ll be able to find the perfect fit for your individual needs, including back braces for work. In a professional setting, the use of a brace may be safer than opioids that could cause you to become dizzy and unresponsive on the job.
Whether you need a back brace for posture for lower back pain, you’ll be able to find the perfect fit for your individual needs, including back braces for work. In a professional setting, the use of a brace may be safer than opioids that could cause you to become dizzy and unresponsive on the job. 3. Get The Correct Size
3. Get The Correct Size  Gestational Diabetes – This type of diabetes occurs during pregnancy and typically develops around the 24th and 28th week. It doesn’t mean you had diabetes before becoming pregnant but does increase your risk for developing type 2 afterward. The exact cause is unknown but pregnancy hormones such as human placental lactogen (hPL) may increase insulin resistance. If not properly managed, gestational diabetes could affect your health, the health of your baby, and impact its birth. Insulin, dieting, and exercise are used to manage this type of diabetes.
Gestational Diabetes – This type of diabetes occurs during pregnancy and typically develops around the 24th and 28th week. It doesn’t mean you had diabetes before becoming pregnant but does increase your risk for developing type 2 afterward. The exact cause is unknown but pregnancy hormones such as human placental lactogen (hPL) may increase insulin resistance. If not properly managed, gestational diabetes could affect your health, the health of your baby, and impact its birth. Insulin, dieting, and exercise are used to manage this type of diabetes. Frequent urination
Frequent urination You will use a glucose meter or glucometer to check your blood sugar level. It works by reading the sugar small amount of blood, usually from your finger, that’s placed on a disposable test strip and you’ll need to record the results. You’ll use a lancet or needle to prick your finger.
You will use a glucose meter or glucometer to check your blood sugar level. It works by reading the sugar small amount of blood, usually from your finger, that’s placed on a disposable test strip and you’ll need to record the results. You’ll use a lancet or needle to prick your finger. Some degree of cognitive decline is natural as a person ages. That said, evidence indicates that staying physically active can help to
Some degree of cognitive decline is natural as a person ages. That said, evidence indicates that staying physically active can help to  Studies indicate that
Studies indicate that 
 So what can be done? Several things, such as X-rays, MRI’s and CT scans, can be done to see exactly what the structures look like; however, be careful – imaging will show you everything going on inside, but doesn’t tell you what’s relevant! As we age, we get wrinkles and gray hair on the outside. The same thing happens on the inside but it’s called “arthritis” and “degeneration.” Further, you can have
So what can be done? Several things, such as X-rays, MRI’s and CT scans, can be done to see exactly what the structures look like; however, be careful – imaging will show you everything going on inside, but doesn’t tell you what’s relevant! As we age, we get wrinkles and gray hair on the outside. The same thing happens on the inside but it’s called “arthritis” and “degeneration.” Further, you can have 
 If something happens to the lymph nodes or vessels, such as damaged caused by surgery, the lymph may become blocks. As a result, it could pull and collect, causing part of your body to swell. While swelling is most common in the legs and arms, it can occur anywhere in the body.
If something happens to the lymph nodes or vessels, such as damaged caused by surgery, the lymph may become blocks. As a result, it could pull and collect, causing part of your body to swell. While swelling is most common in the legs and arms, it can occur anywhere in the body.

 General Enrollment Period – This is your chance to enroll if you miss your initial enrollment period and special enrollment period. The general enrollment period is from January 1st until March 31st and if you enroll during this period coverage will begin July 1st.
General Enrollment Period – This is your chance to enroll if you miss your initial enrollment period and special enrollment period. The general enrollment period is from January 1st until March 31st and if you enroll during this period coverage will begin July 1st.